What about the children?
What about the children?
COVID-19 in children and adolescents A knowledge summary – Version 2 ( from Sweden)
Number of cases among children and adolescents increases with age
A very small proportion of cases have been diagnosed among children up to 6 years of age both in Sweden and globally, but it should be borne in mind that young children have also not been extensively tested. However, slightly more cases are seen as the children get older. With increasing age, a rising number of cases is seen among teenagers, but not as many as among people over 19 years of age. Teenagers seem to be more susceptible to becoming infected than younger children, but experience mild symptoms. Teenagers also transmit the infection to a greater extent than younger children, but to a lesser extent than adults. During October, the number of diagnosed cases increased, especially among older teenagers. A contributing reason for greater transmission among teenagers may be
that they move around more in society and often have many close contacts. The specific role of teenagers in the spread of infection needs to be investigated further through outbreak investigations and infection tracking.
Open Schools, Covid-19, and Child and Teacher Morbidity in Sweden
TO THE EDITOR:
In mid-March 2020, many countries decided to close schools in an attempt to limit the spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus causing coronavirus disease 2019 (Covid-19).1,2 Sweden was one of the few countries that decided to keep preschools (generally caring for children 1 to 6 years of age) and schools (with children 7 to 16 years of age) open. Here, we present data from Sweden on Covid-19 among children 1 to 16 years of age and their teachers. In Sweden, Covid-19 was prevalent in the community during the spring of 2020.3 Social distancing was encouraged in Sweden, but wearing face masks was not.3
Data on severe Covid-19, as defined by intensive care unit (ICU) admission, were prospectively recorded in the nationwide Swedish intensive care registry. We followed all children who were admitted to an ICU between March 1 and June 30, 2020 (school ended around June 10) with laboratory-verified or clinically verified Covid-19, including patients who were admitted for multisystem inflammatory syndrome in children (MIS-C, which is likely to be related to Covid-19)4 according to the Swedish Pediatric Rheumatology Quality Register. (More information on the registry and a link to the World Health Organization scientific brief on MIS-C are provided in the Supplementary Appendix, available with the full text of this letter at NEJM.org.) The Stockholm Ethics Review Board approved the study. Informed consent was waived by the review board.
The number of deaths from any cause among the 1,951,905 children in Sweden (as of December 31, 2019) who were 1 to 16 years of age was 65 during the pre–Covid-19 period of November 2019 through February 2020 and 69 during 4 months of exposure to Covid-19 (March through June 2020) (see the Supplementary Appendix). From March through June 2020, a total of 15 children with Covid-19 (including those with MIS-C) were admitted to an ICU (0.77 per 100,000 children in this age group) (Table 1), 4 of whom were 1 to 6 years of age (0.54 per 100,000) and 11 of whom were 7 to 16 years of age (0.90 per 100,000). Four of the children had an underlying chronic coexisting condition (cancer in 2, chronic kidney disease in 1, and hematologic disease in 1). No child with Covid-19 died.
Clinical trials on children started in March 2021 (for children younger than 12 years old) for the Pfizer-BioNTech vaccine. With total disregard to a warning letter from Dr.Whelan to the FDA, pediatric indication for children 12 -15 was added in the Pfizer-BioNTech vaccine candidate. The clinical trial for this age group was part of the initial Pfizer overlapping clinical trial from November 2020. This with only preliminary results from adult trials. Since May 5, 2021 this vaccine candidate received conditional approval and could therefore now be given to children from this age group in Canada. The terms and conditions of the conditional authorization were updated to include conditions pertaining to children clinical trial results (requirement lines 21 to 24).
Physicians concerns
PEDIACIDE – AN EDITORIAL BY DRS. SENEFF AND PERRO
Note from Drs. Michelle Perro and Stephanie Seneff
The following article is a joint collaboration between Michelle Perro, MD (Executive Director) and Stephanie Seneff, PhD (MIT Research Scientist). In 2017, Dr. Perro and Dr. Adams produced the highly acclaimed book, What’s Making our Children Sick? with a focus on the effects of industrial food on children’s health, highlighting patients’ stories and victories. Dr. Seneff is the author of the about-to-be released, Toxic Legacy, which discusses how glyphosate continues to destroy our children’s health and the environment.
From the GMOScience Team:
This editorial focuses on a different, but equally chilling assault on our children’s health and will further our understanding of what continues to make our children sick. Experimental gene therapy vaccines including both mRNA vaccines and genetically modified DNA vector vaccines are concerning to physicians and scientists.
In 1998, a vaccine was released for infants against rotavirus, a contagious virus that causes diarrhea. Albeit unpleasant, this infectious disease is manageable at home with extra fluids. However, soon after the introduction of the vaccine, it was reported that some infants developed intussusception, a type of bowel obstruction particular to infants where the bowel telescopes in on itself, commonly occurring at the intersection of the small and large intestine. While infants may be quite ill, prompt intervention is curative in all but a few cases.
The risk for development of this bowel obstruction following vaccination was 20-30 times higher than what would be expected in a normal population and occurred within two weeks of the administration of the vaccine. The Centers for Disease Control (CDC), in collaboration with the Food and Drug Administration (FDA) as well as local agencies, quickly intervened and halted the usage of this vaccine. Two emergency investigations were instituted showing that the vaccine increased the risk for intussusception by one to two cases among 10,000 infants who received the vaccine. In response, the manufacturer voluntarily withdrew the rotavirus vaccine from usage in 1999.
The CDC claimed that the decision to remove the rotavirus vaccine was due to the fact that intussusception is a serious condition and that the complications from a rotavirus infection in the US can be prevented by oral rehydration. The CDC states:
“…when a vaccine is discovered to have a serious side effect, a recommendation to continue using the vaccine will be reconsidered and the vaccine may be withdrawn, in spite of the beneficial effect of the vaccine to prevent disease.”
Twenty three years later…
It seems that, in the context of the COVID-19 pandemic, caution has been thrown to the wind. So much about 2020 and the pandemic related to SARS- CoV-2 is unprecedented. In addition to an unprecedented disease and its global response, COVID-19 has also initiated an unprecedented accelerated process of vaccine research, production, testing, and public distribution.
The sense of urgency around combatting this virus led to the creation, in March 2020, of Operation Warp Speed (OWS), then-President Donald Trump’s program to bring a vaccine against COVID-19 to market as quickly as possible, skipping several steps in the normal evaluation process. In response, the National Institutes of Health (NIH) collaborated with the biotechnology company Moderna in bringing an altogether new type of vaccine against infectious disease to market, one utilizing a technology based on messenger RNA (mRNA). Another mRNA vaccine was also developed in parallel by Pfizer in conjunction with a small biotech company in Europe called BioNTech.
Both of these vaccines have been approved for emergency use by the FDA in record time, with little regard for the fact that this technology is experimental and unproven. Now there is an aggressive campaign to get these vaccines into the arms of as many US citizens as possible, also in record time. This is true not only in the US, but also increasingly on a global scale. Essentially, the entire world’s population are serving as guinea pigs in a massive experimental study, and there is clear potential for a great deal of harm.
The global mass vaccination rollout on the world’s adults has now extended its hand into the arms of children. Initially, 16 year olds were encouraged and in some instances, ‘mandated’ to receive the experimental therapy. The age limit has now been decreased to 12 year olds, and imminently 5 year olds and younger are being targeted as the next ‘at risk’ populations. Children have almost zero risk of dying from COVID-19, and it is almost certain therefore that the risk/benefit ratio of these vaccines is too great to warrant their use on children.
To read the entire editorial
Vaccinating children is a crime against humanity

IT IS our moral duty to put the welfare of our children ahead of our own and certainly above that of our parents. This is an inalienable part of what it means to be human: it is nothing less than a prerequisite for survival.
In our response to the Covid-19 virus we have inverted this duty; we have put the welfare of our parents above that of our children. We have imprisoned the young and the healthy, denied them the opportunity to learn and to earn, to socialise and to live full normal lives. We have done this ostensibly to extend the lives of the old and the frail, those with little time left. What have we got from this bargain?
It is far from clear if the lockdown measures have changed the course of the Covid-19 pandemic in any meaningful way. Meanwhile, the old and the frail, those whom the lockdown was aimed at protecting, have been forced to spend the little time they have left enduring half-lives isolated from their friends and families. Have we asked our parents if this is a price they wish to pay? Have we asked our parents if they want those irreplaceable precious years of childhood stolen from their grandchildren, just so they may cower lonely and alone at the end of their lives? We have not, and I, for one, know it is a bargain my parents do not support.
What is worse, far worse, is we are now about to subject our children to a mass immunization program with a new vaccine which has yet to complete its clinical trials and which has been developed, in a hurry, using experimental new technology.
We know healthy young people are either immune to the Covid-19 virus or quickly shake it off. Their natural immune systems protect them. We also know these novel vaccines can have almost immediate devastating life-altering, even life-ending, side-effects for at least a small number of younger people. Importantly, we do not know what the longer-term side-effects of these new vaccines are. We cannot know this because they are new and not yet fully tested.
To administer a new vaccine, developed with new technology, to an entire generation of our children for a disease which they need no treatment for and without knowing its longer-term side effects is unconscionable. A mass vaccination programme of our children, at this time, with these novel vaccines, exposes our children to an unquantifiable and unnecessary risk. Taking such a risk with the health of an entire generation of society is a crime against our children, and a crime against our children is nothing short of a crime against humanity.
We are a matter of weeks away from conducting the riskiest medical experiment in all history. What is more, this experiment is, by its own logic, unnecessary. If the vaccines are effective, as is claimed, it is enough to vaccinate those who are vulnerable to the disease. This has already been done.
For the young and the healthy it is better to allow their immune systems the opportunity to develop their own diverse protections against the disease. Those diverse responses will help protect society against the inevitable evolution of new viruses in the future.
As those who need protecting from Covid-19 are already protected, we now have the time to complete the science calmly and to finish clinical trials of these new vaccines. Only once the vaccines are assessed as safe, in both the short and long run, effective and necessary, should we contemplate mass vaccination of our children. This assessment must be made and be seen to be made using the highest scientific standards. It cannot be done without open scrutiny of the data and a robust debate about its interpretation.
Science is the process of challenging accepted wisdom. This can be done only within a society which tolerates vigorous debate and open dissent. We cannot follow the science, on Covid-19 or any other issue, if we do not tolerate, listen to, and learn from those with whom we disagree. In the last year it has become increasingly difficult openly to dissent from the government’s chosen path on dealing with the Covid-19 virus. It is time to reclaim our rights to free speech, open debate and yes, at times the right to offend the opinion of others.
We will make mistakes if those who doubt the wisdom of a course of action are not encouraged to speak out. Today, those who doubt the wisdom of inoculating our children with these new experimental vaccines are being discouraged from speaking out. When free speech stops, great mistakes follow.
*******************************************
Adverse reactions in young patients after SARS-Cov-2 vaccine candidate injection
Risk of death from the vaccine
Data pertaining to serious adverse event in children need to be regularly consulted before deciding to inject or not.
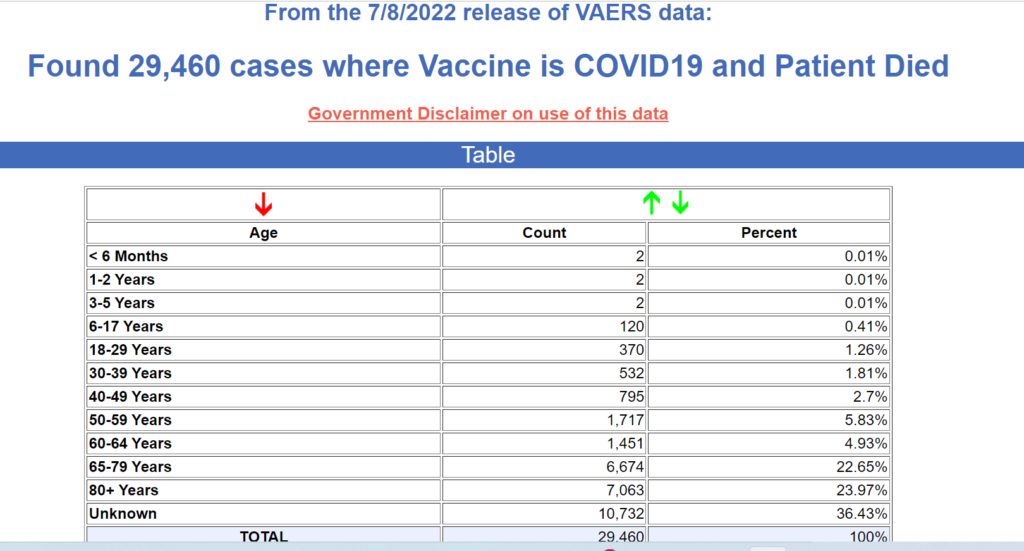
For an auto-updating table of death after anti-covid injection for the young demographic 6 month to 25years old ( weekly update)
Some are considering giving this injection to older children without parental consent; in Quebec, Canada, children aged fourteen and up will not need parental consent to be injected. They are encouraged to go with friends to drive-through inoculation sites as if going for some fast food pickup. With the complexity of the issues at hand, how could children give informed consent to an intervention that has the potential to forever change their life, when they just barely learned to read and write?
These mandates and pressure raises serious legal and ethical concerns. Who is there to protect the children? The medical body around the world has sounded the alarm on many occasions.
Although the completion date for the phase 1-3 clinical trials is estimated to be in May 2023, from March to June 2021, thousands of children and teenagers were injected with the Pfizer product against SARS-Cov -2 virus. Moderna is also conducting clinical trial in preparation for the rollout in the pediatric clientele. Due to increasing data reporting evens of myocarditis and pericarditis in this young group, the WHO issued a cautionary statement about vaccinating the young people in the society: WHO: ‘Children Should Not Be Vaccinated for the Moment’
Share and donate
Share your experience with family and friends.